 What is Capsular Contracture?
What is Capsular Contracture?
One of the most popular and commonly performed cosmetic procedures, breast augmentation involves inserting an implant within the breast to achieve the desired contour. Complications after the procedure are rare; however, they can occur from time to time. While in most cases they can be corrected if treated early, the importance of educating yourself so you can seek timely treatment cannot be overstated.
As with the introduction of any non-biologic material into the body, once a breast implant is in place, scar tissue forms around it inducing the formation of a tissue capsule. This harmless capsule, usually soft and pliable, is part of the healing mechanism and helps hold the implant in place. In some patients, though, this tissue capsule becomes unusually hard and dense, and starts to constrict the implant, causing pain and aesthetic distortion of the breast. This condition, known as Capsular contracture, is the most common complication associated with breast augmentation.
What are the signs and symptoms of this condition?
This condition can occur at any time; however, it often begins within months after the procedure. It is characterized by several symptoms that can develop over time. These may include:
- An increasing feeling of pain, tightness, or discomfort in the breast; this pain is typically exacerbated when lying flat on your stomach.
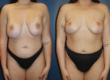
- Distortion or change in the shape of the breast; the breast may have a ball-like shape or show visible rippling.
- Displacement in the position of the breast; the breast may appear to sit higher on the chest than normal after having settled into its final position, creating a dissociated breast look.
- Deformity in the appearance of the breast; the breast may look misshapen or unnatural.
What are the possible causes?
Capsular contracture can occur regardless of the type of breast implant placed in your breast. While a definitive cause for this condition remains elusive, there are some common potential factors.
- Bacterial infection: The formation of a bacterial biofilm in the breast pocket, generally introduced during the insertion of the implant in the breast cavity, is known to play a potential causative role.
- Hematoma and Seroma: Undrained hematomas and seromas are known to contribute to the condition by providing a nutrient-rich environment for the growth of microbial biofilm.
- Genetics: A family history of autoimmune diseases or a genetic predisposition to developing thick scar tissue could also be a risk factor.
Is it possible to prevent the development of this condition?
While it is impossible to eliminate the probability of developing this condition, it is possible to minimize the risk if you and your surgeon work together on certain strategies during and after the procedure.
- The surgeon’s role: Your surgeon may use prophylactic measures such as administration of antibiotics before and antibiotic irrigation during the procedure; use of “under the muscle” placement and minimal handling of the implant, use of drains to inhibit the formation of biofilm from hematoma or seroma; and use of postoperative antibiotics until the removal of drains.
- Your role: You can do your part in lowering the risk by avoiding vigorous activity and preventing any kind of trauma to the breast after the procedure; doing the required exercises and massage as instructed by the doctor; and attending regular checkups.
What are the treatment options available for capsular contracture?
Both nonsurgical and surgical options are available to treat this common complication of breast augmentation surgery.
The nonsurgical treatment involves shock wave therapy which uses external high-intensity sound waves to help soften and break up the hardened scar tissue. A fairly new development, this noninvasive option is typically found to be effective with early contracture and might not work for everyone.
The surgical option is often the standard treatment for moderate to severe contracture. There are different types of surgical procedures to address this condition.
- Capsulotomy: A simpler option, the contracture has a higher rate or recurrence with this procedure. During this procedure, the thickened tissue capsule is cut open and internally released so that it does not squeeze the implant tightly. The implant, however, stays in place. Capsulotomy can be open or closed. Open surgery entails an incision in the breast to access the capsule, while closed surgery uses external compression to break up the capsule and is rarely performed anymore.
- Capsulectomy: In this more invasive procedure, the scar tissue capsule is surgically removed. The implant itself is also usually replaced. Capsulectomy can be subtotal or total. In subtotal capsulectomy, only a portion of the capsule is removed, while in total, the entire capsule is removed. A third type of capsulectomy – en bloc capsulectomy – involves the removal of the capsule and the implant as one intact unit and is reserved for select cases. Total capsulectomy is shown to produce the lowest rate of subsequent contracture.
- Introduction of Acellular Dermal Matrix (ADM): A modern alternative in treatment options, introduction of ADM during the procedure may be an effective tool in preventing contracture recurrence. In this procedure, sheets of decellularized dermal tissue are used to create a pocket for the implant. This matrix is believed to redirect the way collagen is laid down, thereby preventing the capsule from contracting the implant.
Capsular contracture can be very uncomfortable and potentially compromise your overall quality of life. However, it is easily treatable. If you notice any of the signs, call your surgeon as soon as possible.